
Case 3
A 62-year-old man was brought to Emergency Department for severe chest tightness of sudden onset, lasting 30 min. He had experienced episodes of chest tightness unrelated to exertion for one year.

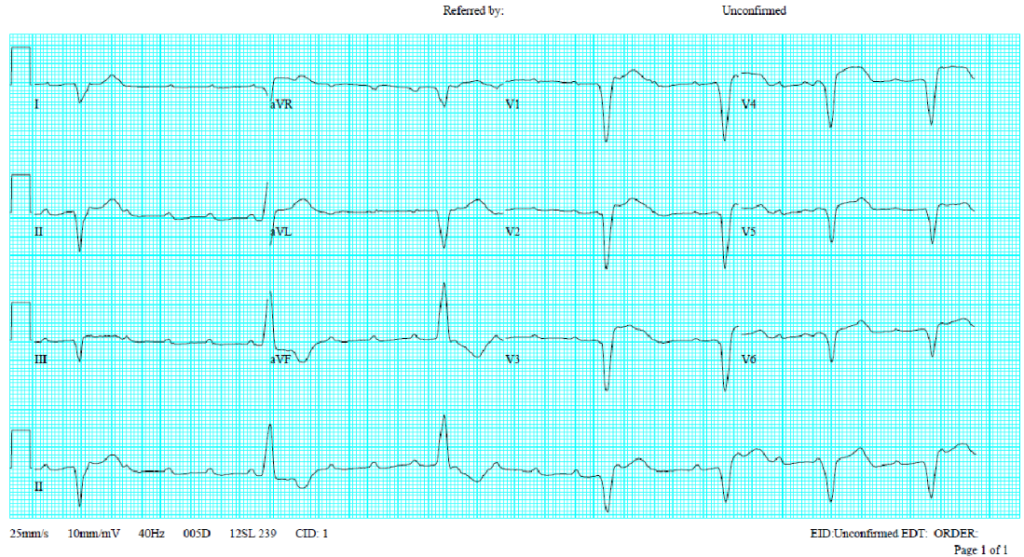
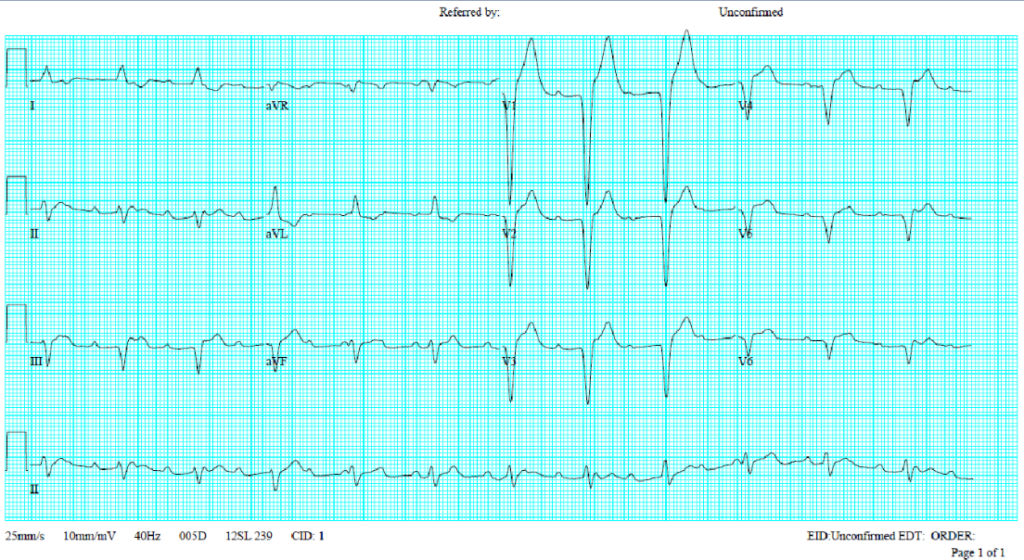
A 62-year-old man was brought to Emergency Department for severe chest tightness of sudden onset, lasting 30 min. He had experienced episodes of chest tightness unrelated to exertion for one year.

A 30-year-old woman, a professional cook, suddenly experienced retrosternal chest tightness after dinner, which increased in intensity without radiation, lasting for 2 hours.

Case 34 Content When this 78-year-old man walked into the clinic, he looked weary and depleted. For the past two days, he had been battling an intermittent fever topping 37.8°C, accompanied by a vanis