The previous pacemaker system was removed.
Clinical interpretation
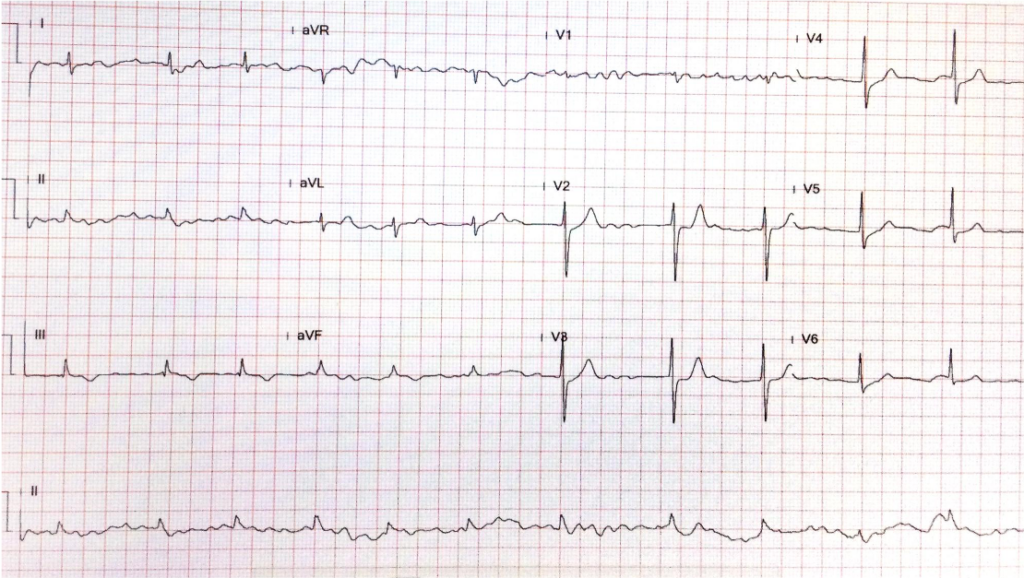
Despite having staphylococcus aureus endocarditis, characterized by positive blood cultures and valvular vegetations on echocardiography, the average ventricular rate of chronic atrial fibrillation in this patient measures only 70/min. During the initial clinic visit, the physician did not suspect a severe disease due to the absence of tachycardia and leukocytosis (6500 /uL). It appears that the patient’s response to infection, including sympathetic tone and immune reaction, is delayed due to their old age, which accounts for the “subacute” clinical presentation. There is also a possibility that associated atrioventricular nodal dysfunction, which is also related to old age, or adrenergic beta-receptor blocking agent therapy (not present in this case) may mask the tachycardia response in patients with severe infectious illness.
Pacemaker-induced bacterial endocarditis is an infection affecting the heart’s inner surface or valves. This infection can be caused by bacteria that enter the bloodstream during the implantation of a pacemaker or afterward. The presence of vegetation on the mitral and aortic valves (the left side of the heart) is a sign of hematogenous bacterial spread. Staphylococcus aureus is the most common pathogen found in these types of infections, but other bacteria like coagulase-negative staphylococci, streptococci, and enterococci can also cause the disease. The symptoms of the infection can occur suddenly (acute form) with high fever, chills, and systemic illness or have a more gradual onset (subacute form) with fatigue, weight loss, loss of appetite, and other nonspecific signs, especially in older patients.
Blood cultures and echocardiography confirm the diagnosis of this type of endocarditis. Managing pacemaker-induced infectious endocarditis involves antibiotic therapy and removing the infected hardware, including the pulse generator and pacing lead. However, removing the pacemaker system may cause further hematogenous spread of bacteria, as illustrated in the present case, so careful management is crucial.
The blood culture results typically guide antibiotic treatment and require consultation with an Infectious Diseases specialist. Prevention measures are also essential in clinical practice and include good hand hygiene, aseptic device handling, and prophylactic antibiotics before the procedure if necessary. Careful follow-up and monitoring for signs of infection in patients post-procedure. In high-risk patients, such as those with cancerous diseases, receiving immunosuppressive agents or previously infected implantable cardiac electronic devices, an absorbable antibacterial envelope and preprocedural intravenous antibiotics postprocedural oral antibiotics (e.g., pre-op: cefazolin 1 to 2 g IV; post-op: cefazolin 2 g IV TID for one day followed by ciprofloxacin 250 to 500 mg PO BID for seven days) are strongly recommended.
The development of hyperthyroidism during this case is intriguing. Although stress or an infectious process can provoke hyperthyroidism in the present case, clinicians should also consider other possibilities, such as excessive iodine consumption, which can lead to an overactive thyroid in susceptible individuals. This can occur through the Jod-Basedow phenomenon, a thyrotoxic state caused by iodine-containing compounds in patients with pre-existing autonomously functioning “thyroid nodules,” as this patient has.
While the bulk of the literature does not directly associate typical antibiotics with the induction of hyperthyroidism, a specific subset of antibiotics loaded with a significant amount of iodine, known as iodinated glycerol, can exacerbate thyroid function in susceptible individuals. Other well-known medications can provoke or exacerbate hyperthyroidism, such as amiodarone, interferons, lithium, and thyroxine.
Amiodarone is an iodine-rich drug used for arrhythmias that can cause both hypothyroidism and hyperthyroidism. Amiodarone-induced Thyrotoxicosis is associated with an excess iodine load that leads to increased synthesis of thyroid hormones in an abnormal thyroid gland (Jod-Basedow phenomenon). However, it can also cause destructive thyroiditis, leading to the release of preformed thyroid hormones from normal glands.
Interferons and other immunomodulatory drugs commonly used for treating multiple sclerosis and Hepatitis C may trigger autoimmunity, including Graves’ Disease. Lithium, while more commonly associated with hypothyroidism, can induce hyperthyroidism through its inhibiting effect on the release of thyroid hormones. This results in goiter formation with subsequent leakage of large amounts of thyroid hormone, causing “leak-induced” hyperthyroidism. It is noteworthy that these drugs do not induce hyperthyroidism in everyone, and they generally occur in individuals who already have an underlying thyroid condition, such as “thyroid nodules” or autoimmune susceptibility. Lastly, Over-replacement or misuse of levothyroxine can cause iatrogenic hyperthyroidism, which is not uncommonly seen in clinical practice.
*Gallium-67 citrate scintigraphy is a nuclear medicine imaging study based on the principle that gallium-67 (67Ga), a radiotracer, binds to transferrin and other proteins of iron metabolism. Once attached, inflammatory cells, particularly neutrophils and macrophages, take up these, which can be imaged. This technique can detect abscesses, osteomyelitis, lung infections, and certain malignancies. However, while gallium scans can be beneficial in detecting certain conditions, they do not provide the same anatomical detail as a CT scan. Therefore, they are often used with other imaging modalities for a more comprehensive evaluation. The test also has a relatively high radiation dose and a long acquisition time.
Intravenous contrast media used in computed tomography (CT) are typically iodine-based compounds. These contrast agents enhance the visualization of specific tissues or blood vessels during CT imaging. Currently used are non-ionic monomers or dimers. 1. Non-ionic monomers: These are low-osmolality contrast media (LOCM). They are now the most commonly used type of intravenous contrast in CT. 2. Non-ionic dimers: These are iso-osmolality contrast media (IOCM). They have the same osmolality as human blood, which can reduce the risk of adverse reactions. However, they are more expensive than LOCM. Most iodinated contrast media for CT scans contain 300-370 mg iodine/mL. The higher the iodine concentration, the greater the radiopacity and the better the enhancement of the tissues during imaging. The total amount of iodine administered to a patient during a CT scan depends on its concentration and the volume of the contrast medium dispensed. It’s important to note that the use of iodinated contrast media can carry risks, including allergic reactions and “contrast-induced nephropathy,” particularly in patients with pre-existing renal impairment. Therefore, the decision to use contrast and the choice of contrast agent should be made on an individual patient basis, considering the potential risks and benefits.
**Gentamicin-induced renal dysfunction (nephrotoxicity) is characterized by acute kidney injury (AKI), which can manifest as decreased urine output, elevated serum creatinine, and abnormal electrolyte levels. The diagnosis is primarily clinical, based on the temporal relationship between gentamicin administration and the onset of renal dysfunction. Laboratory tests play a crucial role in the diagnosis. These include monitoring serum creatinine (Cr) levels, blood urea nitrogen (BUN), and electrolyte levels. Urinalysis may show proteinuria and the presence of renal tubular epithelial cells.
In some cases, a renal biopsy may confirm the diagnosis, but this is usually reserved for cases where the diagnosis is unclear. The primary treatment for gentamicin-induced nephrotoxicity is the discontinuation of the drug. This often leads to improvement in renal function, although recovery may take weeks to months, and in some cases, the damage may be irreversible. Supportive care is also essential, which includes maintaining adequate hydration, correcting electrolyte imbalance, and avoiding other nephrotoxic agents (e.g., contrast media for imaging). In severe cases, renal replacement therapy (dialysis) may be required. The use of certain medications like N-acetylcysteine and sodium bicarbonate has been studied for the prevention and treatment of aminoglycoside-induced nephrotoxicity. Still, the evidence is not strong enough to recommend their routine use. Prevention is critical in managing gentamicin-induced nephrotoxicity:
- Using the lowest effective dose.
- Monitoring drug levels to avoid toxic peak and trough levels.
- Limiting the duration of therapy.
It’s also important to closely monitor renal function in patients receiving gentamicin, especially those with risk factors for nephrotoxicity, such as advanced age, pre-existing renal disease, and concomitant use of other nephrotoxic drugs (e.g., gentamicin and CT contrast medium in the present case).
***CPAP has several effects on cardiopulmonary circulation. Firstly, CPAP improves oxygenation by increasing the functional residual capacity, reducing breathing work, and improving gas exchange, thereby benefiting obstructive sleep apnea, HF, and acute respiratory distress syndrome. Secondly, CPAP can reduce preload and afterload on the heart. By increasing intrathoracic pressure, CPAP decreases venous return to the heart, thereby reducing preload, favoring conditions like HF, where the heart is overloaded. On the other hand, by improving oxygenation and reducing hypoxic pulmonary vasoconstriction, CPAP can decrease pulmonary artery pressure and thus reduce the afterload on the right heart. Thirdly, CPAP can have a positive effect on LV function; CPAP can improve LV ejection fraction in patients with HF by reducing preload and afterload. However, it’s important to note that while CPAP can have beneficial effects on cardiopulmonary circulation, it can also have potential adverse effects. For instance, increased intrathoracic pressure can decrease venous return and cardiac output, particularly in hypovolemic patients. Therefore, careful patient selection and monitoring are necessary when using CPAP.
****Novel oral anticoagulants (NOACs) variably depend on renal clearance. Their dosages should be adjusted according to serum creatinine. Individual patient characteristics (e.g., age, body weight, etc.), comorbidities, and concomitant medications (i.e., drug interaction) should be considered when choosing and dosing a NOAC. Always refer to the specific prescribing information for each drug and consider consultation with a pharmacist or specialist in anticoagulation when managing these patients. Generally, with age ≥80 years, body weight ≤60 kg, or serum creatinine ≥1.5 mg/dL, the recommended dose for stroke prevention in AF should be reduced to half of the standard dosage. Rivaroxaban is eliminated by metabolic degradation through the liver (approximately two-thirds) and by direct renal excretion of unchanged compound (about one-third of the administered dose). Therefore, it was reasonable for the care team to reduce the dosage of rivaroxaban from 15 mg to 10 mg per day in the present case.
Keywords: complications of pacemaker implantation, drug-induced kidney
Injury, infective endocarditis, Jod-Basedow phenomenon