
Case 13
This 30-year-old woman complained of having had about ten episodes of syncope associated with mild exertion for the past six months.


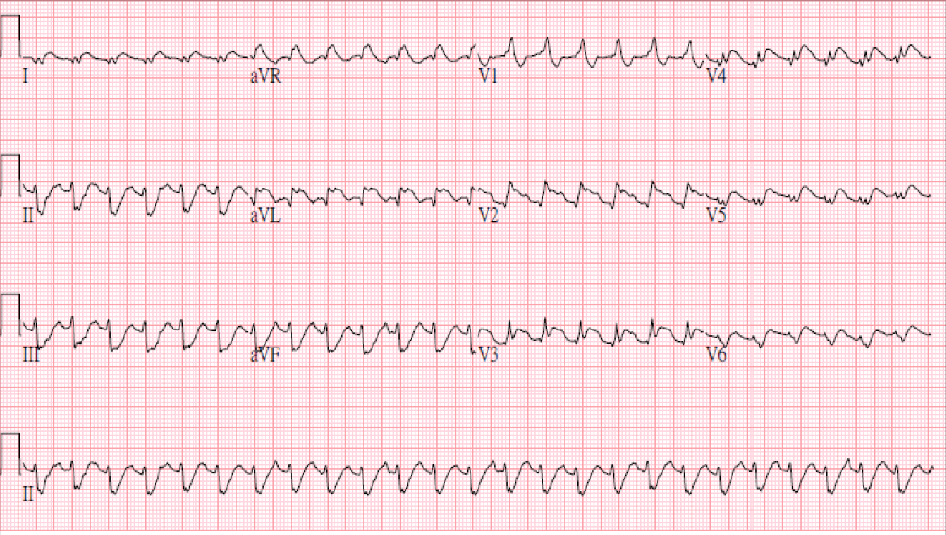

This 30-year-old woman complained of having had about ten episodes of syncope associated with mild exertion for the past six months.
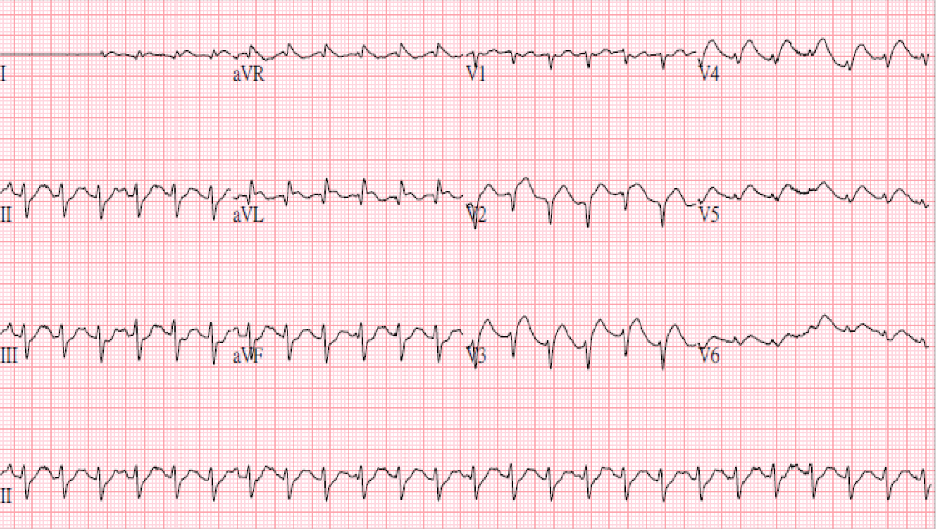
A 38-year-old man was admitted because of having abdominal fullness associated with progressive SOB (PND and orthopnea) for ten days. He denied having abdominal pain,
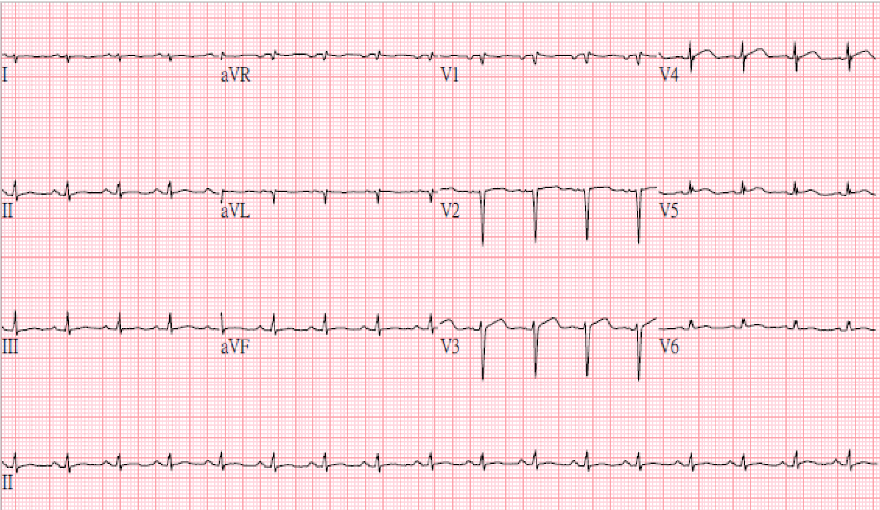
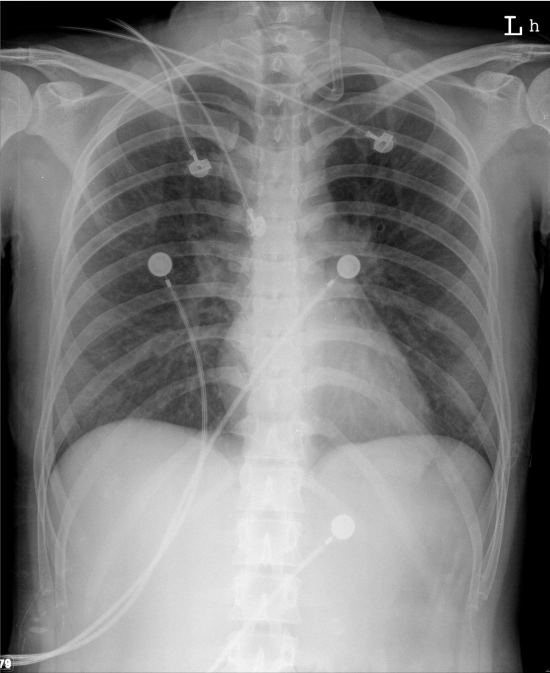
A 43-year-old woman, s/p mitral valve (MV) replacement (Bjork-Sheily) for mitral stenosis (MS) associated with rheumatic heart disease 18 years ago, was admitted with worsening