Case 11
A 38-year-old man was admitted because of having abdominal fullness associated with progressive SOB (PND and orthopnea) for ten days. He denied having abdominal pain, chest pain/tightness, fever, cough, or palpitations.


A 38-year-old man was admitted because of having abdominal fullness associated with progressive SOB (PND and orthopnea) for ten days. He denied having abdominal pain, chest pain/tightness, fever, cough, or palpitations.
An 81-year-old man came to the Emergency Department (ED) after one day of having progressive dyspnea with orthopnea and had diffuse itchy skin for more than a week.
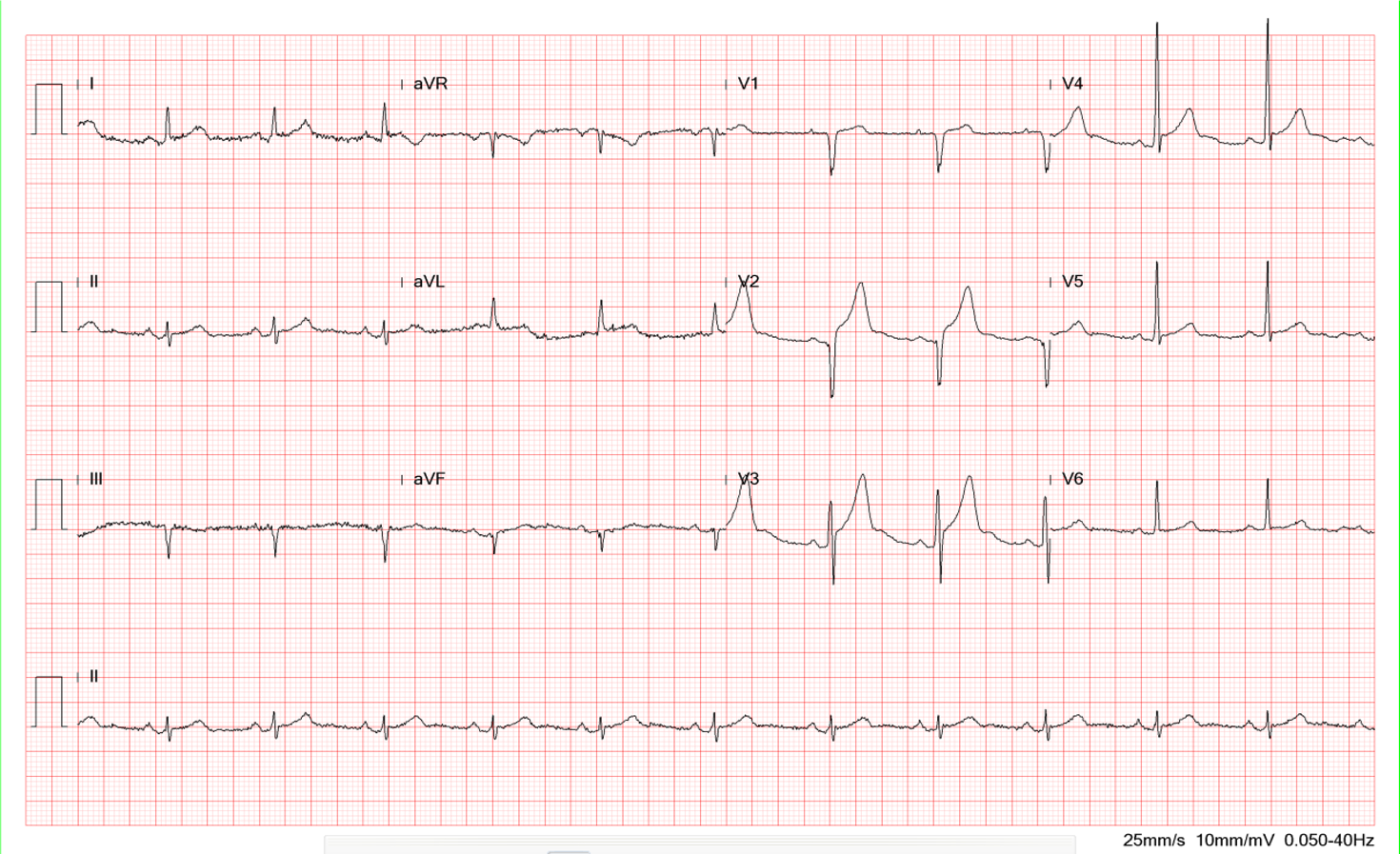
This 50-year-old man came to the Emergency Department complaining of having substernal chest pain for more than 10 hours. The pain was sharp and not exertion-related. It could radiate to the left shoulder, back, and scapula. It seemed positional, as inspiration could worsen it, and leaning forward could somewhat mitigate the pain. At times, he also experienced nausea, dyspnea, and cold sweats. Reportedly, he had flu-like symptoms with a runny nose and sore throat but didn’t visit any clinic seeking help. Past medical history was significant for thalassemia, mild GERD, and gallbladder stone diagnosed ten years ago.