
Case 13
This 30-year-old woman complained of having had about ten episodes of syncope associated with mild exertion for the past six months.

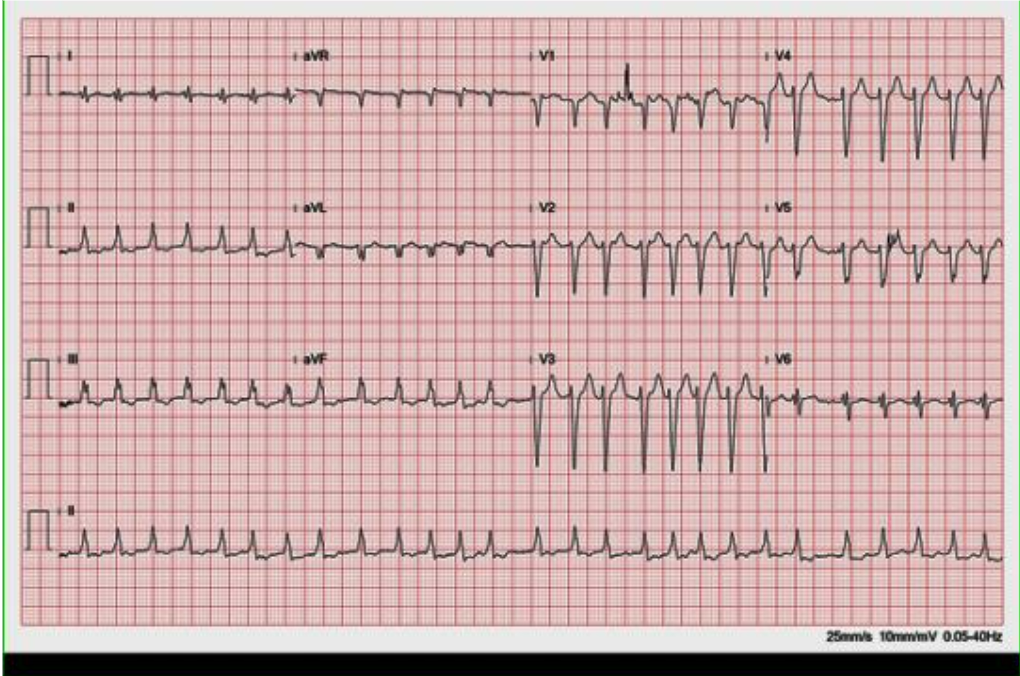

This 30-year-old woman complained of having had about ten episodes of syncope associated with mild exertion for the past six months.

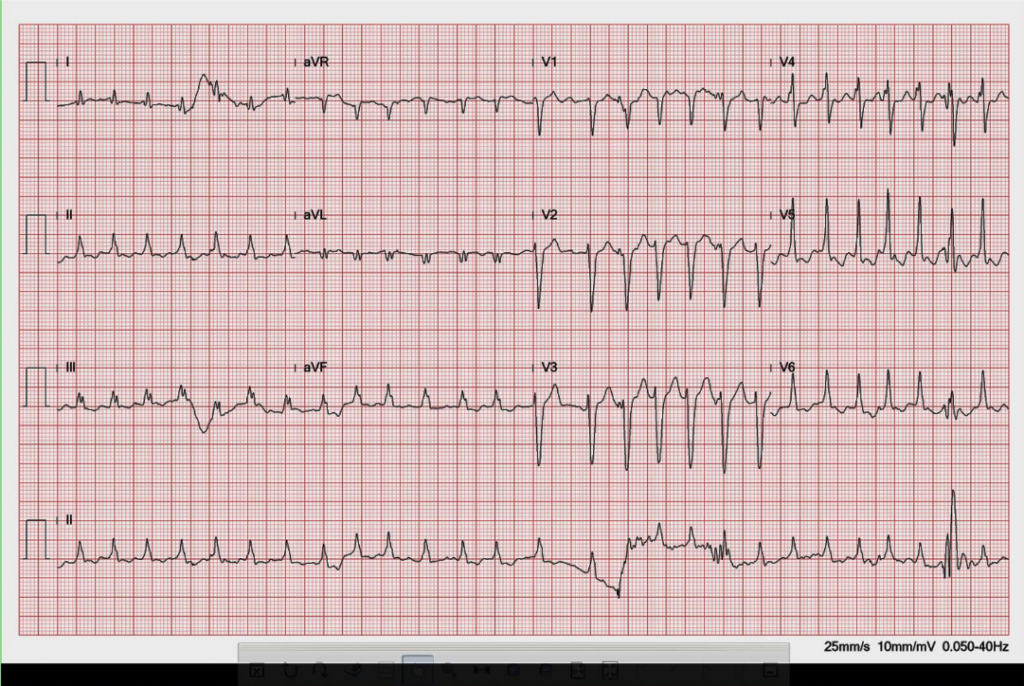
A 62-year-old man was brought to Emergency Department for severe chest tightness of sudden onset, lasting 30 min. He had experienced episodes of chest tightness

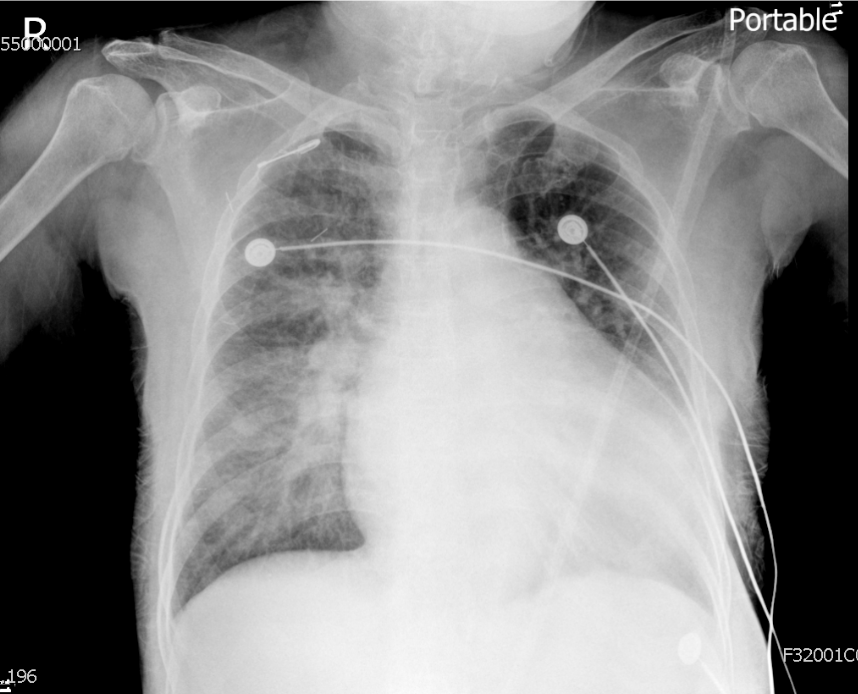
An 88-year-old woman complained of a loss of appetite, generalized weakness for two weeks, and increasing SOB for five days. She had chronic heart failure