
Case 8
A 65-year-old man was brought in with progressive edema of the left arm below the elbow level for two weeks. It was not “red and hot” but painful. In addition, he noted leg edema, PND, and increasing SOB on exertion.

A 65-year-old man was brought in with progressive edema of the left arm below the elbow level for two weeks. It was not “red and hot” but painful. In addition, he noted leg edema, PND, and increasing SOB on exertion.

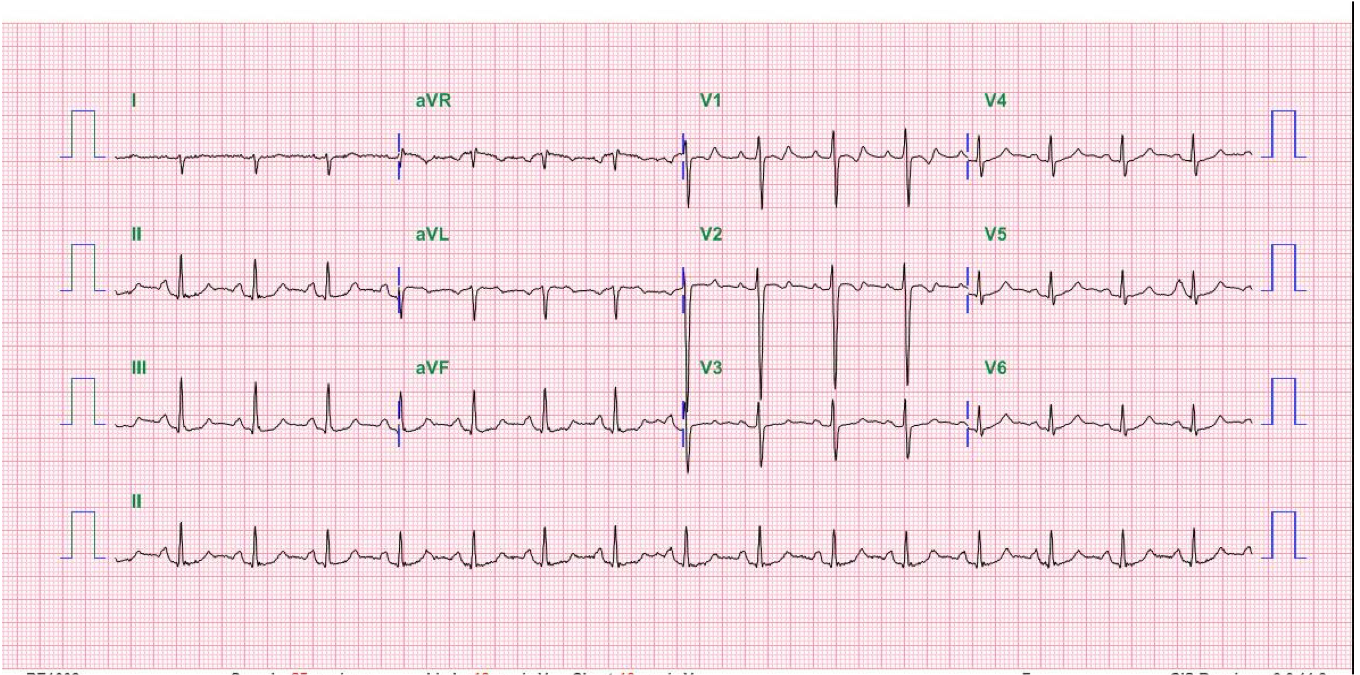
This 30-year-old woman complained of having had about ten episodes of syncope associated with mild exertion for the past six months.
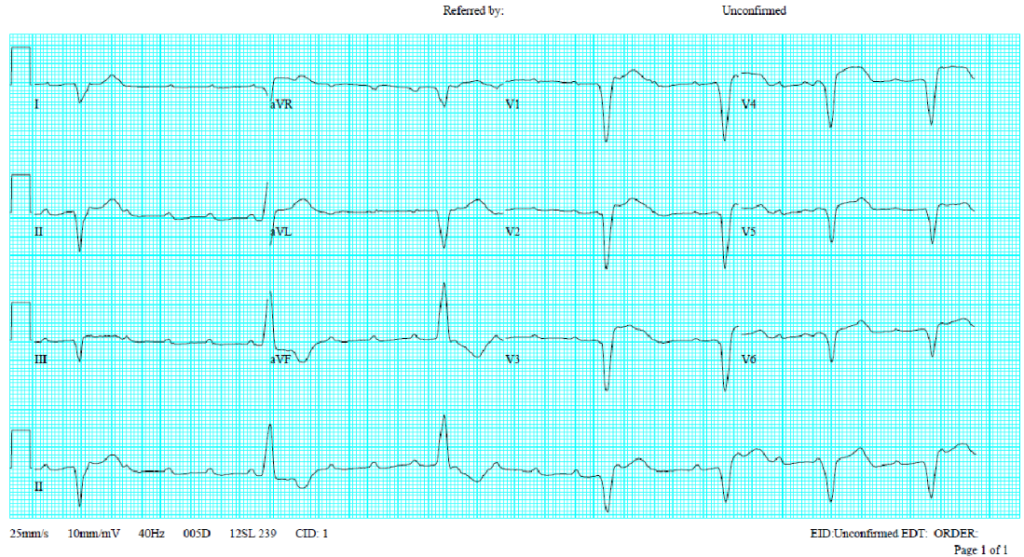
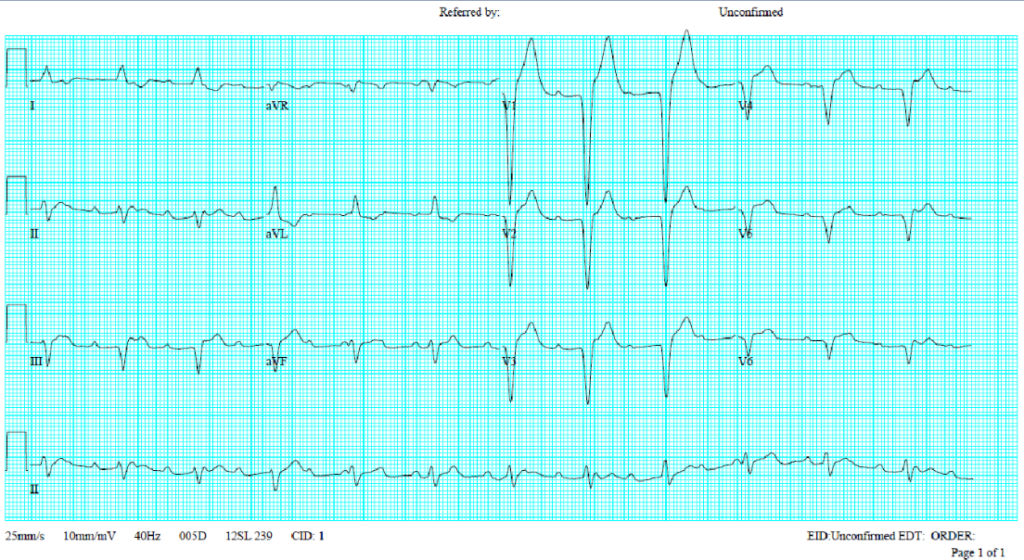
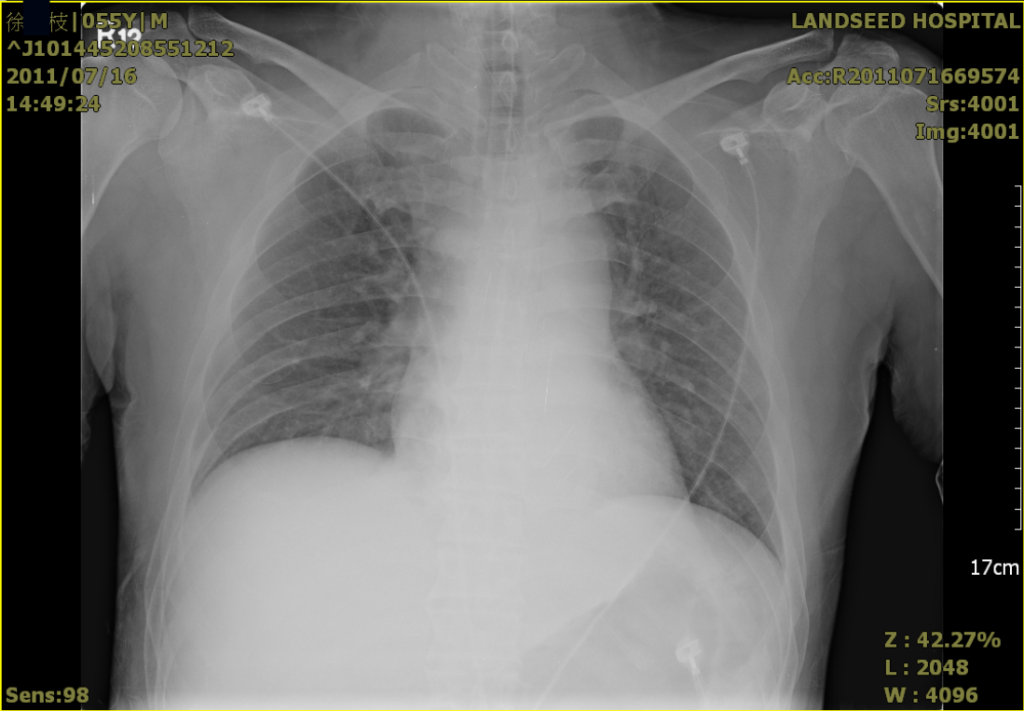
A 52-year-old man was admitted because of progressive dyspnea on exertion for one week. In the past, he had chronic obstructive pulmonary disease (COPD), alcoholic liver cirrhosis with minimal esophageal varices, gastroesophageal reflux, and duodenal ulcer with bleeding but no hypertension, diabetes mellitus, or atherosclerotic coronary heart disease (CHD). He was one pack a day smoker and a daily drinker for at least 25 years.