Case 18
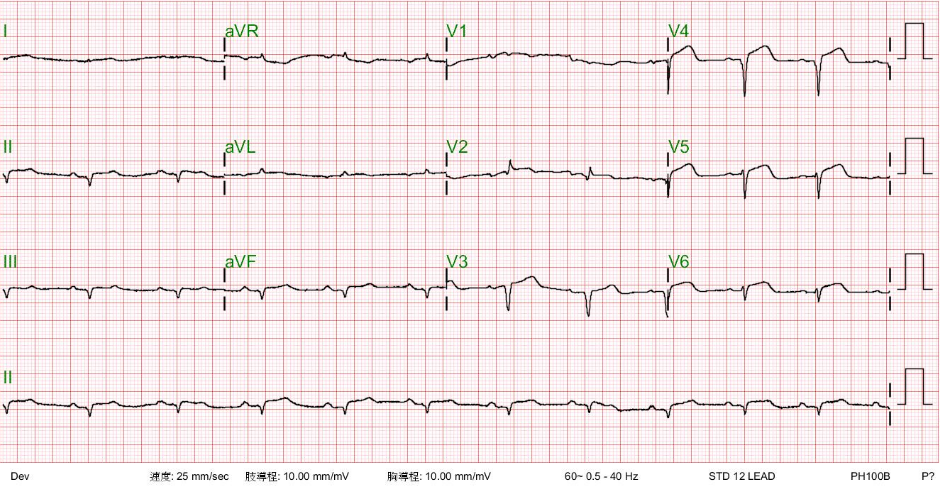
This 69-year-old man had been in good health until two days before admission when he returned from a beach. He experienced general weakness with chest

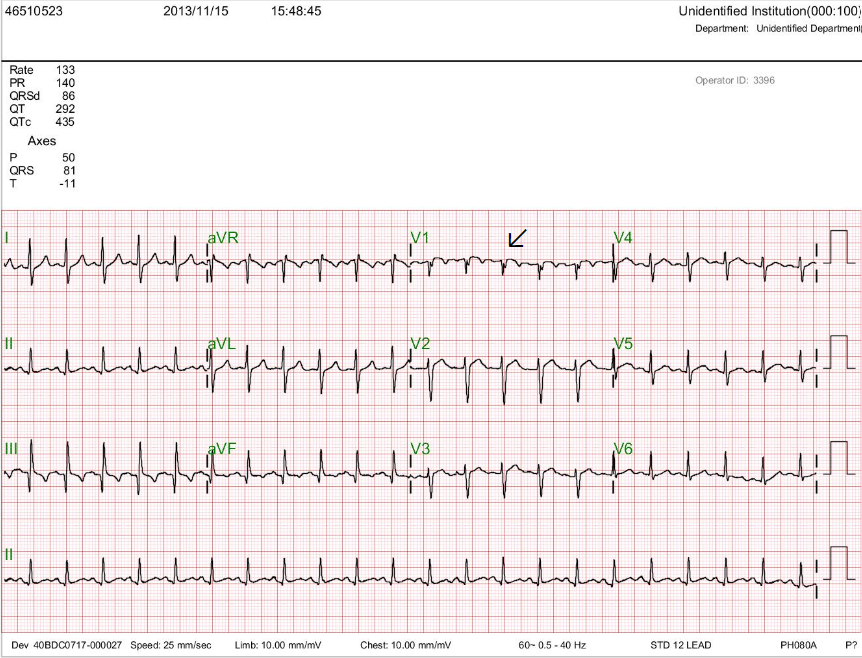

This 69-year-old man had been in good health until two days before admission when he returned from a beach. He experienced general weakness with chest

A 62-year-old man was brought to Emergency Department for severe chest tightness of sudden onset, lasting 30 min. He had experienced episodes of chest tightness
This 35-year-old male was transferred from a local hospital for further evaluation after a biopsy of a hard, 4 cm in diameter lymph node in