
Case 13
This 30-year-old woman complained of having had about ten episodes of syncope associated with mild exertion for the past six months.

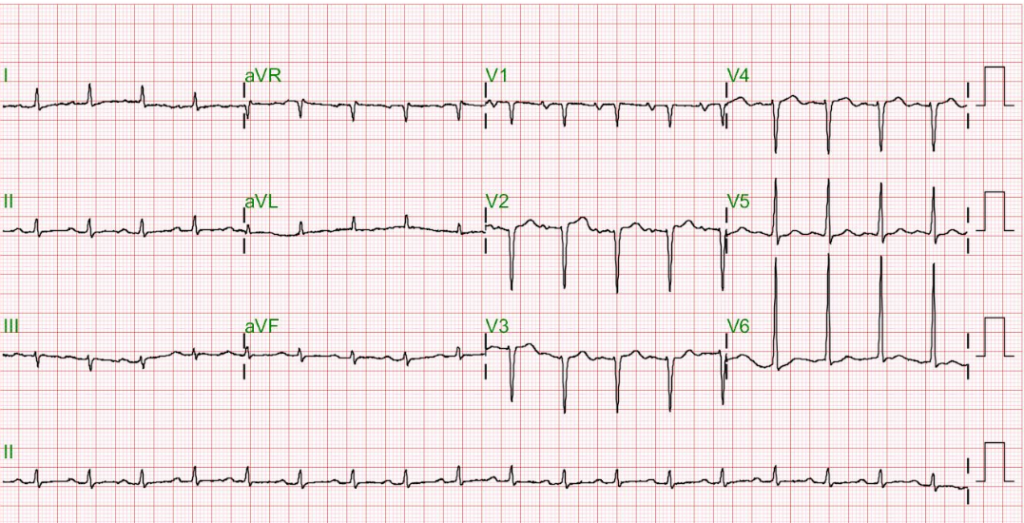


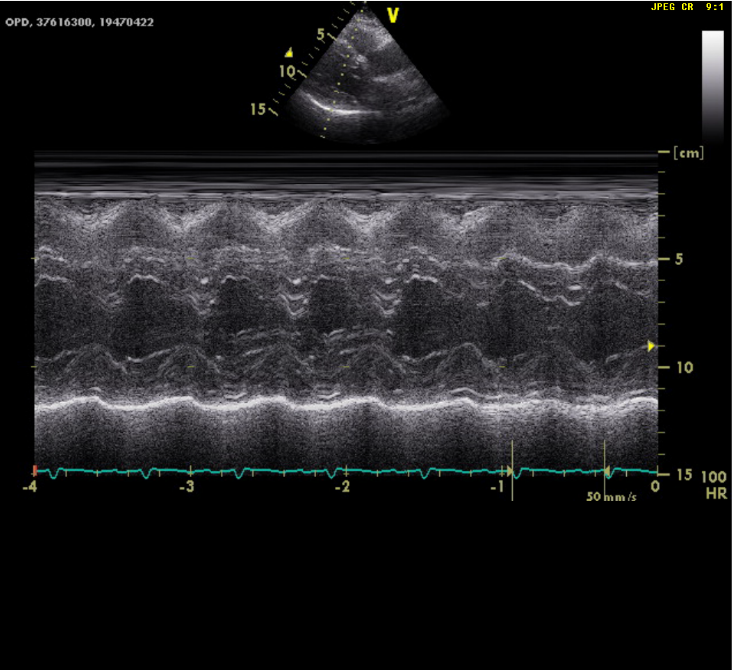
This 30-year-old woman complained of having had about ten episodes of syncope associated with mild exertion for the past six months.
A 38-year-old man was admitted because of having abdominal fullness associated with progressive SOB (PND and orthopnea) for ten days. He denied having abdominal pain,
This 43-year-old woman was rushed to ER because of the sudden onset of substernal chest tightness accompanied by cold sweats, which lasted more than 30